CBCT 3D training: From cone beam to surgical guide
15 janvier 2025Clear Aligners: Alternative to Conventional Orthodontic Systems
20 mars 2025
The Digital Set-Up in Orthodontics
Certainly, the application of digital technologies in orthodontics is relatively recent. However, the rise of digital technology is inevitably leading us into a new era of orthodontic practice.
Digital workflows are now an integral part of our daily activities in modern dentistry.
Indeed, these digital technologies are present at every stage. From the acquisition of optical impressions to 3D printing using stereolithography, the production of custom-made orthodontic aligners, and the digital set-up.
The digital set-up is a prime example of how digital tools enhance orthodontic treatment.
Historical Overview
It all began in the late 1990s, when a group of young American engineers developed a computer software capable of virtualizing dental arches and simulating individualized tooth movements, thus enabling the correction of malocclusions and dental malpositions with aligner trays.
This marked the birth of the modern digital set-up.
Align Technology, with its Invisalign aligner system, was the first company to successfully manufacture appliances based on a digital set-up.
Definition of a Digital Set-Up
Generally speaking, a set-up is a visualization of a possible post-treatment situation.
A digital set-up is the 3D modeling, via specialized software, of dental and gingival movements, allowing the pre-visualization of the different steps of orthodontic treatment up to the final result.
This computerized animated set-up serves mainly as the basis for treatments using aligners—transparent thermoformed trays aimed at correcting dental malpositions.
Its main objective is to help choose the most suitable therapeutic solution for the clinical situation while minimizing treatment duration.

Figure 1 / Digital Set-Up
Creating the Digital Set-Up
Starting from optical impressions taken directly in the mouth, scanned impressions, or scanned models, the software (e.g., ClinCheck by Invisalign, Approver by Spark) creates a virtual final model based on the practitioner’s directives.
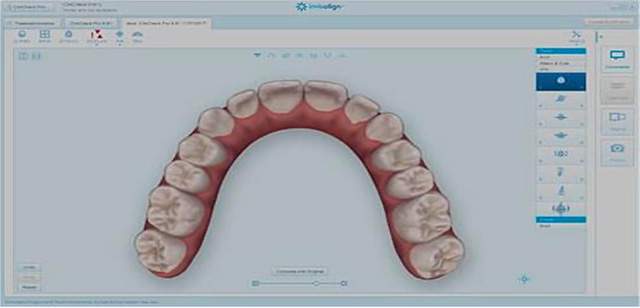
Figure 2 / Invisalign CLINCHECK Software Interface
The dento-alveolar units are separated individually and then repositioned in the working digital model.
Once the axis, position, and contact points of the teeth, as well as the gingival outline, are reproduced virtually, the treatment plan is applied, and the movements are sequenced in a video by the software.
In treatments involving clear aligners, this step of movement sequencing—pre-visualizing the sequence of each individual tooth movement—requires particular attention.
The practitioner receives an initial treatment simulation to which they can make any desired changes.
They can thus preview each movement individually, each therapeutic step, or the entire treatment as a whole.
The software makes it possible to group together in a single step those movements that complement each other and to postpone opposing movements to later stages. For example, transverse expansion and lingual tipping of the incisors work very well together, generating exactly the same deformation of the aligner.
It is also important to observe how quickly tooth movements are occurring because it is possible to accelerate a specific movement using treatment auxiliaries (for instance, wearing elastics at night or wearing them continuously throughout the day).
With remarkable precision, the software visualizes the magnitude of each tooth’s movement in three spatial planes and determines the amount of interproximal enamel reduction or stripping, when needed, with the possibility of creating multiple treatment plans.
The software also allows you to request different treatment scenarios and receive multiple set-ups in order to compare them and choose the most appropriate treatment plan for the clinical situation.
This can help the practitioner decide whether to treat the case with or without therapeutic extractions or whether to perform interproximal reductions, etc.
Once the virtual alignment is completed, the practitioner determines the number of stages needed for the final correction. Since dental movements must be performed gradually, each step involves only a few degrees of rotation or a few tenths of a millimeter of movement.
Each step corresponds to a virtual model generated as an STL file by the system.
Each digital file is then 3D printed to serve as a model for creating the individualized thermoformed trays in the dental laboratory.
Traditional (Manual) Set-Up vs. Digital Set-Up
Traditionally, the laboratory technician would cut the teeth out of the plaster model and reposition them in wax in an optimal position.

Figure 3 / Traditional Set-Up
This simulation allows the evaluation of potential therapeutic objectives such as performing stripping (interproximal enamel reduction) or therapeutic dental extractions.
In 1956, Kesling used the traditional set-up to finalize his orthodontic treatments and later for treatment planning and orthodontic diagnostics.
The digital set-up is based on the same principles as the manual set-up. However, in the digital approach, the separation of the teeth is done via a very precise digital procedure, unlike the standard plaster model cutting, which damages the tooth structure in plaster.
In the digital model, teeth are segmented using virtual segmentation techniques. For example, in 3Shape software, the segmentation process begins by placing a point on the mesial and distal sides of each tooth in the virtual model. This marking can be done semi-automatically, but the user’s manual validation is required.
The software then draws a segmentation line along the gingival margin, separates the tooth crowns from the gingiva, and defines interproximal contacts.
In the digital set-up, the shape of the arch is individually defined by software tools, whereas it is based on a predetermined shape in the traditional set-up.
Advantages of the Digital Set-Up
- Creating a digital set-up is much less time-consuming than performing a manual set-up.
- The digital set-up is done in front of a screen and is therefore far more flexible than a classic plaster set-up.
- Modifications to the virtual digital model can be made infinitely and saved, whereas with a manual set-up, any modification is irreversible.
- The procedure for digitally separating (segmenting) the teeth increases accuracy compared to cutting teeth out of plaster.
- In a digital set-up, the arch shape is established individually for each case, unlike the standard laboratory-based approach.
- The digital set-up can be easily saved, eliminating the need for plaster models and the associated storage problems.
- Dental movements are exceptionally precise and can be easily evaluated using an overlay of tooth positions with color coding to compare initial and final tooth positions.
- The most advanced software now also allows superimposing the set-up on digital radiographs, combining virtual models (STL files) with DICOM files (Digital Imaging and Communication in Medicine) from Cone Beam Computed Tomography (CBCT).
For example, with Ormco’s Insignia® system, combining optical impressions and CBCT acquisition makes it possible to evaluate root parallelism, bone thicknesses, or the alveolar corridor, thus considering both tooth crowns and roots when planning tooth movements.
Indeed, conventional multi-bracket treatments with buccal brackets have also benefited from these digital advancements. Their design can now be fully individualized: the bracket slot data can be customized, and the orthodontic wires can be made to measure as well.
Ongoing progress in digital technologies has evolved these systems since their inception to increase predictability and therapeutic effectiveness.
It is now possible to precisely quantify the extent of the intended movements. Thanks to the use of Big Data—collecting and critically analyzing which movements are achieved and which are not with aligners—movements that are at the limits or impossible to achieve are now better detected.
The digital analysis of this data has led to system improvements, such as optimized attachments, and to expanding the system’s range of applications.
This is a valuable asset for the prescribing practitioner, enabling them to better anticipate the need for various accessories to achieve the desired movements (e.g., choice of dental attachments, intermaxillary elastics, mini-screws, or combined bonded brackets). It also allows for planning any stages that might be combined with traditional orthodontic approaches.
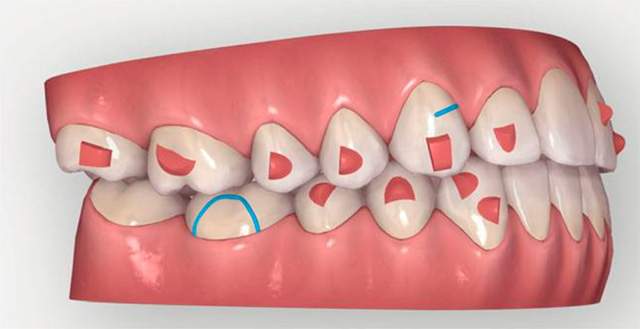
Figure 4 / Example of Movement Auxiliaries: Dental Attachments
Thanks to digital technology, the practitioner has ever-greater control over planned treatments. They can create, visualize, and modify different set-ups without incurring additional costs. The entire diagnostic–set-up–aligner fabrication chain can be partially or even fully carried out in the dental office.
The practitioner is no longer dependent on a single set-up proposed by the laboratory technician, and communication with the technician is much smoother and more straightforward.
The set-up also facilitates communication between the orthodontist and the patient.
Patients can easily preview their orthodontic treatment with the practitioner, as well as the final result. This is especially helpful in cases where an extraction may be necessary. The set-up serves as a tool to explain the reasoning behind this choice and helps patients better accept their treatment.
Furthermore, by using these digital tools for orthodontic treatment planning, it is now possible to virtually compare the planned tooth movements at a given time with the patient’s actual orthodontic situation. This makes it possible to more objectively monitor and evaluate the patient’s orthodontic progress, much like a digital monitoring system.
The Limitations of Digital Orthodontics
We must acknowledge that digital set-ups are virtual tools and do not incorporate all the environmental factors needed when developing a comprehensive treatment plan—such as dental anchorage (determined by the clinical crown/clinical root ratio and facial type), the sagittal and frontal relationships of the jaws, lip closure, smile line, etc.
A set-up is useful for showing the patient the various stages of treatment. However, it is crucial to explain that teeth do not move exactly the way they do on a computer screen, as they are part of a living biological system.
Even with precise detection of movements that are more or less predictable, it remains vital to respect certain biological and biomechanical principles governing tooth movement within the alveolar bone and the musculoskeletal system.
For instance, excessive expansion or uncontrolled constriction may lead to inappropriate or unstable results, and in some cases, periodontal complications such as recessions, dehiscences, or tooth mobility.
Prefabricating orthodontic appliances, such as clear aligners, based on digital set-ups can limit the practitioner's ability to make quick adjustments in unexpected clinical situations.
Conclusion
Digital orthodontic treatment planning tools are cutting-edge technologies that enable practitioners to visualize different set-ups, superimpose tooth movements, and overlay digital impressions with radiographic images. They also allow the visualization of aligner “morphing” sequences.
Predictability is a major asset of the digital set-up, as it allows for highly accurate quantitative analysis of tooth movements.
However, repositioning teeth and making orthodontic corrections must always consider the far more complex skeletal and muscular systems—not just the virtual model viewed on a computer screen.
For this reason, it is essential that a practitioner trained in these digital tools and techniques oversee the set-up, as they alone can determine whether the virtual tooth movements programmed on the computer are truly achievable in the mouth, taking into account periodontal conditions, occlusion, and the type of appliance used, among other factors.
Orthodontic software tools continue to evolve every day, looking increasingly toward the future—especially through the use of Big Data and the advent of Artificial Intelligence in dentistry.
Figure 2 / Invisalign CLINCHECK Software Interface
Les unités dento-alvéolaires sont séparées individuellement et ensuite réintégrées au modèle de travail numérique.
Une fois que l’axe, la position, les points de contact des dents ainsi que la situation de la gencive sont reproduits virtuellement, le plan de traitement est appliqué et les mouvements sont mis en séquence vidéo par le logiciel.
