3d Printing in dentistry – Owandy Radiology
13 January 2025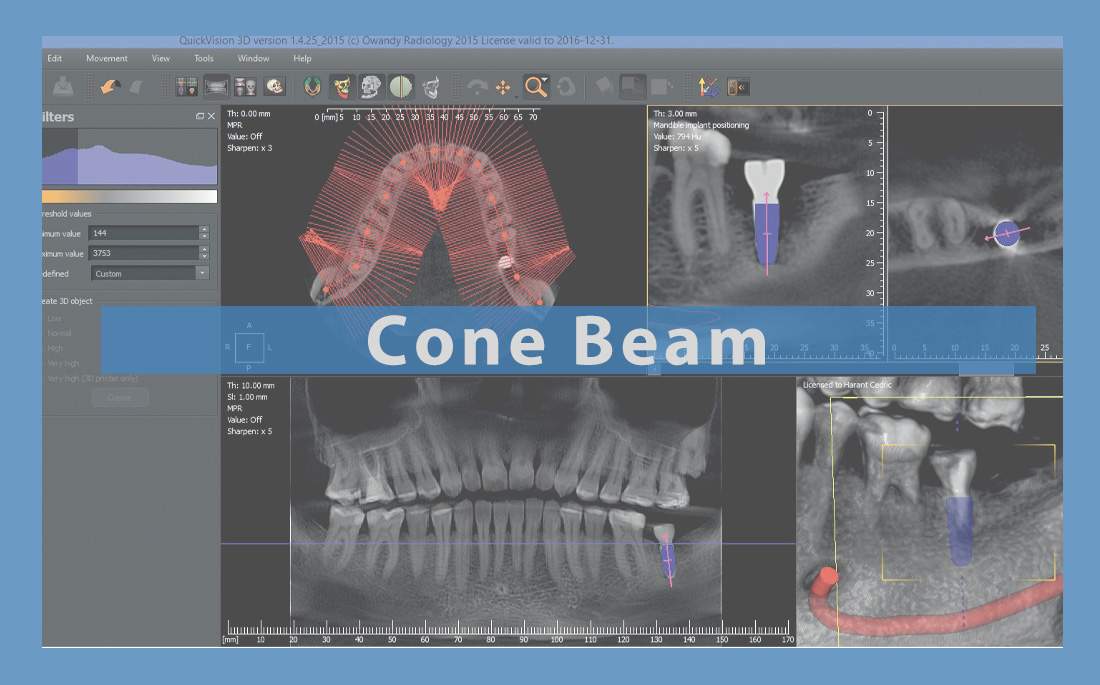
CBCT : Cone beam computed tomography for dental implants surgery
Introduction
Establishing an accurate dental implant diagnosis involves a painstaking clinical examination, often supplemented by additional radiological exams.
Cone Beam or CBCT (Cone Beam Computed Tomography), and also known as digital cone beam volumetric tomography, is a rapidly growing 3D sectional imaging technique. It can be harnessed to explore calcified tissues, i.e. bones and teeth.
This article will be examining this revolution in dento-maxillary imaging, which has been widely adopted in dental surgeries, opening up new horizons for diagnostics in dentistry.
Firstly, we’ll be defining Cone Beam technology and explaining the physical principle of this radiological process. We’ll then briefly review the differences between scanners and Cone Beam CT, followed by a discussion of the benefits and limitations of CBCT, still in comparison with scanners. Lastly, we’ll look at the clinical indications for use of this technique.
What is CBCT technology?
Definition
We can identify two different types of technique in dento-maxillary imaging: 2D panoramic or orthopantomographic (OPT) techniques, and more sophisticated 3D techniques such as scanners and, more recently, CBCT.
The advent of CBCT towards the end of the 1990s was seen as a major innovation in comparison to its predecessor, the scanner, as it introduced large scale matrix detectors that could scan a complete volume in just one rotation of the imaging system.
How does CBCT work?
Physical principle
As its name suggests, CBCT comprises an x-ray generator that emits an open conical radiation beam for sweeping the whole volume to be explored in a complete or semi-complete rotation, before being analyzed once the detection system has recorded it. The x-ray generator and detector are interdependent and aligned.
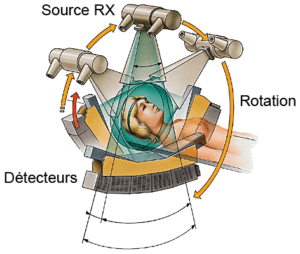
Figure 1 Physical principle of TDM
x-ray tube / conical x-ray beamflat sensor
With each rotational degree, the generator releases a pulse of x-rays that pass through the anatomical mass so that they are received by the detector, which then carries out a rotation at the same time as the source.
With each angular motion, a 2D image of the volume covered is recorded on the flat sensor.
Digital acquisitions take hundreds of images so that a volume can be created and 3D computer reconstruction can deliver a virtual view of the anatomical structures explored.
Tube / Object / Detector / Digitalization / Image memory / Reconstruction / Image processing / Console / Film / Digital image acquisition

Figure 2: Principle of 3D CBCT image reconstitution
Unlike with scanners, each unit or Voxel is isometric, creating a very high spatial resolution of around 100µ.
CBCT can be used to obtain a volumetric image of the area x-rayed, with a high image resolution for the various dimensions, by eliminating any overlapping of surrounding structures.
There are various types of CBCT, categorized according to their field of investigation:
– small fields: less than or equal to 8cm
– medium fields: between 9 and 15cm
– large fields: greater than 15cm
What happens in a CBCT dental examination?
The session is similar to that of a standard dental x-ray. The patient must stay motionless throughout the acquisition time, which lasts around 10 to 20 seconds. A computerized reconstruction is then carried out using dedicated software. Around 20 to 30 minutes is required for each examination, which is considerably more than the time taken by a scanner.
What is the radiation dose of a CBCT exam?
Cone Beam technology uses very different technical solutions, with radiation doses in ratios of 1:5.
It is defined by dosimetric studies as being the least irradiating of all sectional techniques. Cone Beam exposure doses are 1.5 to 12 times weaker than those used by conventional medical scanners. However, they are still 4 to 42 times stronger than panoramic imaging.
As a guide:
| Technical | Intra-oral image | Panoramic image | Cone beam |
| Absorbed radiation dose in Gray | 1 to 8 mGy | 3 to 7 mGy | 3 to 25 mGy |
The CBCT technique complies with the ALARA (As Low As Reasonably Achievable) principle set out in national radioprotection legislation, which stipulates that the weakest dose necessary should be applied.
CBCT versus Scanners
Just like its predecessor, the scanner, CBCT is used to obtain 3D reconstitutions but is technically quite different.
Below is a table comparing both techniques
The main technical differences between Cone Beam CT and Scanners
| Scanner | CBCT |
| Flat x-ray beams (fan-shaped) | Conical open x-ray beams |
| Linear, slim sensor | Flat sensor |
| Imaging requires multiple rotations around patient | Fast imaging requiring just one rotation |
| Standard equipment design (patient must be lying down) | Standard design similar to OPT, where patient is standing |
| Cuboid voxel: anisotropic volume | Cubic voxel: Isotrope volume |
| Radiation +++ | Radiation + |
Because of these different techniques, CBCT offers some genuine advantages compared with the scanner. Let’s take a look at some of the main ones.
What are the advantages of CBCT compared with scanners?
Patient comfort
The image acquisition process is easier, quicker and more comfortable for the patient, who no longer needs to lie down but instead can simply stand up, as with panoramic images. The equipment only needs to rotate once around the patient.
Dosimetry and radiation
Unlike scanners, CBCT is considered to be a “low dose” technique, capable of sweeping the entire volume to be explored in one go, while also being less irradiating than conventional tomodensitometry.
CBCT delivers an ionizing radiation dose up to 6 times weaker than that from the same exam conducted by a scanner.
Below is a table comparing effective doses used in the main odontostomatological radiological processes.
| Source | Average effective dose |
| Digital retro-alveolar image | 4 to 6 uSv |
| Digital panoramic radiography | 10 to 15 uSv |
| Medical scanner | 60 to 1300 uSv |
| Cone beam | 20 to 250 uSv |
CBCT can be used to identify the investigation field in the area to be studied (a dental sector, or full arch, for example), thereby avoiding needlessly irradiating other parts of the skull.
Image options, spatial resolution and clarity
CBCT can be used to obtain a range of different views from the same image, i.e. frontal, sagittal, coronal and oblique sections.
Cone Beam produces isotropic voxels of between 500μm and 75μm, with an enlargement ratio of 1:1, which can be used to refine analysis of bone and dental structures as well as deliver a high resolution capability in various dimensions that is similar – and, in some cases, superior – to that of the scanner.
Sensitivity to artefacts
Cone Beam CT is less vulnerable to metal artefacts than the scanner is, particular in terms of the root zone.
Cost
CBCT is considerably cheaper than the scanner.
What are the limitations of Cone Beam compared with the scanner?
Image acquisition and console operation
While the CBCT is acquiring the images, the patient is in a standing position. This makes it difficult to remain immobile for the entire rotation time of the device (20 to 30 secs). There is a considerable risk of movement, which could result in kinetic artefacts. Because of the relatively long image acquisition time compared with that for a scanner, all Cone Beam equipment should include an effective immobilization system designed to reduce this risk of movement that is virtually non-existent in TDM (where the exposure time is extremely short – around 6 seconds).
Furthermore, Cone Beam examinations take longer to reconstruct 3D images.
Signal to Noise ratio, and density / contrast resolution
The higher the Signal to Noise ratio, the better the density resolution. Cone Beam delivers a low contrast resolution compared with scanners, because of its lower Signal to Noise ratio.
While Cone Beam CT offers a superior resolution to that of dental panoramic imaging and scanners, its density range is much smaller because of its low radiation. The image quality it produces is insufficient to measure the density of calcified tissues and analyses soft tissues, which limits its usage.
The advantages of Cone Beam CT are already well acknowledged across all fields of dento-maxillary imaging.
What are the indications for Cone Beam CT?
In this article, we’ll be limiting ourselves to CBCT applications in odontology, maxillo-facial imaging and ORL.
Odontostomatology
CBCT has a role to play in odontostomatology should the information created by the clinic and conventional 2D radiology (intra-oral and OPG images) prove insufficient for the purposes of establishing an accurate diagnostic, and when a 3D image is essential:
In implantology
Thanks to its biomeasurement qualities, and the accuracy it is able to deliver because of its isotropic characteristics that ensure exact linear measurements, CBCT has a natural role to play in biometric-focused implantology. The possibilities it offers for bi and tri-dimensional reconstructions, navigation, and surgical simulation, coupled with its low sensitivity to metal artefacts, constitute additional welcome assets for implantology.
It can be used to establish a pre-op diagnostic report after a standard clinical and radiological examination of the patient, in order to advise implant placement in the event of any doubt, or to establish a contraindication, and – in some cases – post-surgical monitoring. It can be used to provide an accurate measurement of the available bone volume on the implant site and provide the best possible view, as well as a quantitative and qualitative bone study after assessing the density.
It can also measure distances to assess the proximity of anatomical structures to be avoided, such as nerves and sinuses, for the purposes of implant placement.
3D modelling can be carried out to virtually simulate the placement of any future implants, by selecting the appropriate size and shape.

Figure 3 – Digital implant planning with QuickVision 3Dv
The sectional imaging delivered by Cone Beam TC is more than an elective implantology examination; it can be a compulsory examination except in cases where implant treatment is contraindicated by clinical examinations and OPT.
We owe the development of static and dynamic guided surgery to CBCT techniques, which have also made it easier to process 3D anatomical data.
Guided implant surgery involves placing the patient’s mouth impression (.stl file) over the radiological data derived from the Cone Beam (DICOM file) using dedicated software. It is now possible to optimize the accuracy of surgical tasks, thereby minimizing the number of failed implant treatments that occur in conventional surgery, and pushing the limits of oral implantology.
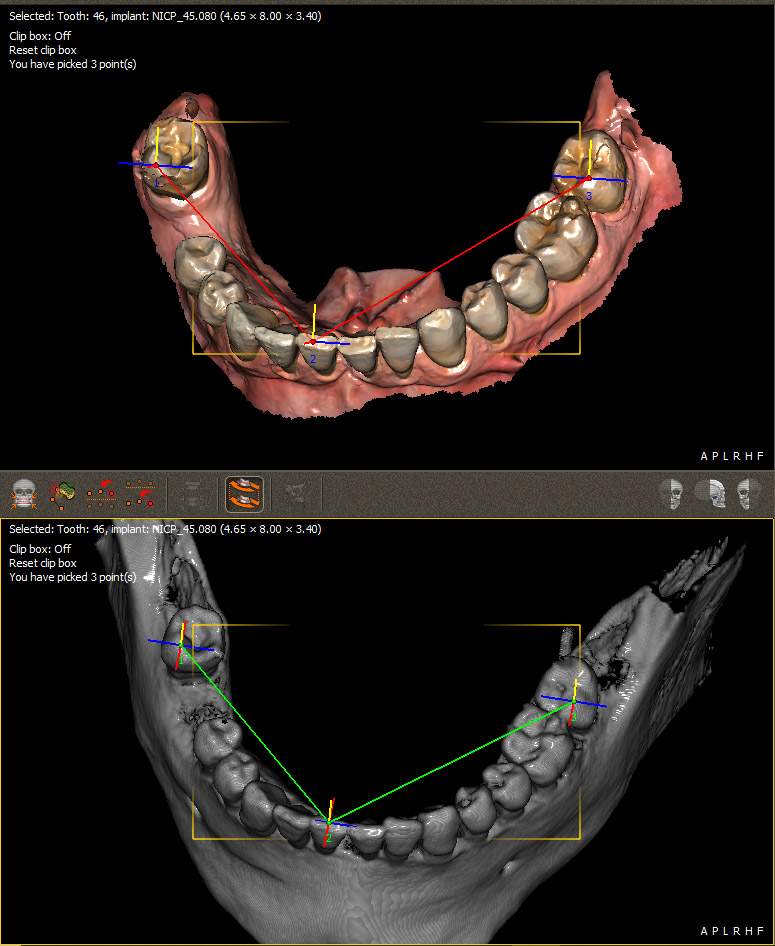
Figure 4 Matching STL and DICOM files using QuickVision 3D
In terms of therapeutic follow-up, this mainly involves clinical and 2D radiological processes, but if there is the slightest risk of complication (immediately defective osteointegration, peri-implantitis, etc.) following implant placement or after a pre-implant treatment by graft, or a sinus lift, then the use of CBCT should not be ruled out.
Conservative odontology and endodontics
Cone Beam is particularly useful for researching and identifying additional root canals, for peri-apical pre-op reports, particularly in the posterior maxillary region or the posterior mandibular region in the mental foramen area.
It is also useful in cases of alveolo-dental traumas, for determining the type of fracture and assessing radicular pathology (fractures, internal and external resorption, peri-apical or lateral-radicular, etc.).
In oral surgery, particularly prior to extracting impacted teeth and wisdom teeth, in order to see where the roots are in terms of the inferior alveolar nerve.
In pathology, to draw up a further assessment and identify the links between cystic and tumor lesions in maxillary bones.
ORL and maxillo-facial
Cone Beam CT can also be used in ORL and maxillo-facial treatments. It primarily enables exploration of nasal sinuses and nasal cavities, and surgical navigation with pre-op imaging using endoscopic sinus surgery, and can also compile a pathology report on TMJs (temporomandibular joints). It is also suitable for exploring the middle ear, to assess pathologies, as well as for post-operative monitoring of hearing implants.
A few recommendations
Cone Beam CT is a first-line examination for inflammatory and infectious pathologies affecting nasal sinuses.
Cone Beam CT is a third-line examination for dento-maxillary imaging (after intra-oral imaging and OPG).
Choosing the right Cone Beam equipment
Choosing the right Cone Beam imaging device depends on the specifications. Some perform better in terms of implantology, while others are more geared towards pathology and oral surgery diagnostics, or endodontics.
Conclusion
A cross between the dental panoramic unit and the scanner, CBCT is characterized by its unique ability to read higher densities, with a greater degree of accuracy than OPT, and enjoying better spatial resolution than TDM. It also offers the option of low-cost 3D digital reconstitution, while being less invasive than the scanner.
Its technical and dosimetric performances have seen Cone Beam CT prove the ideal choice in almost all areas of odontostomatology, periodontology, oral surgery, orthodontics and even endodontics.
It is currently prescribed whenever soft tissue examinations are not required, and when a 3D image is essential. It is used to diagnose TMJ lesions, bone cysts and tumors, traumas, and infections; however, its low density and contrast resolution makes it less suitable for exploring soft tissues.
Cone Beam is currently recognized as the leading sectional imaging process in odontostomatology, hence the need to make it widely available.
However, it should not be prescribed automatically, as it should really be considered as an additional examination to complement conventional 2D and clinical radiology.